Week of:
Bridging the Collaboration Gap: New Math in the Clinical Trials System
October 9, 2017
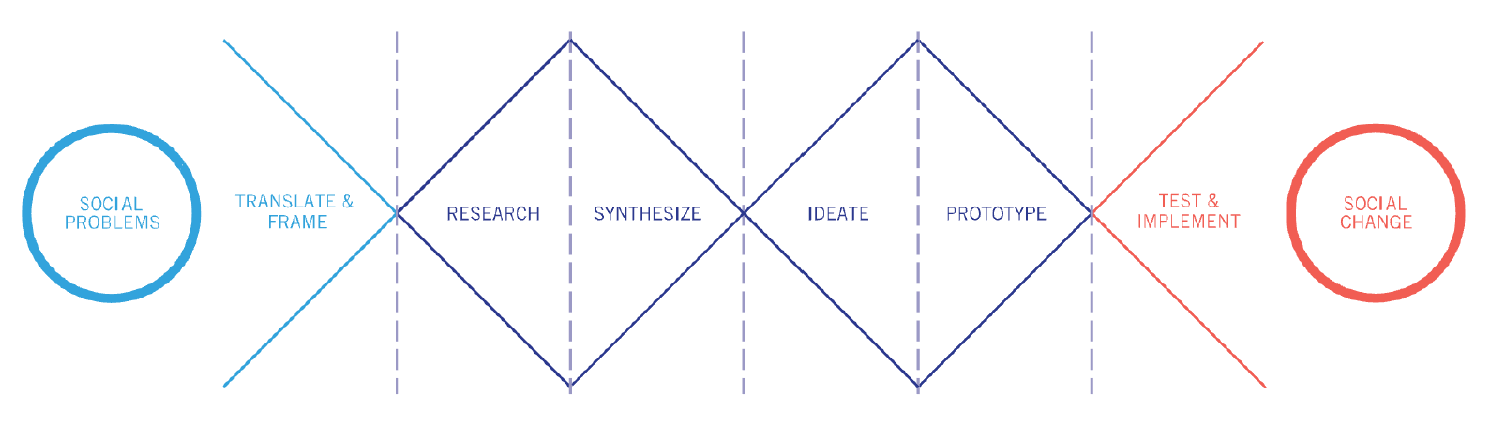
Our next recommendation tackles a critical methodological gap in medical research. We propose to facilitate the collaboration of pure mathematicians with clinical trial researchers so that they can continuously develop new mathematical techniques that are relevant to the modern challenges in the treatment development system.
Background
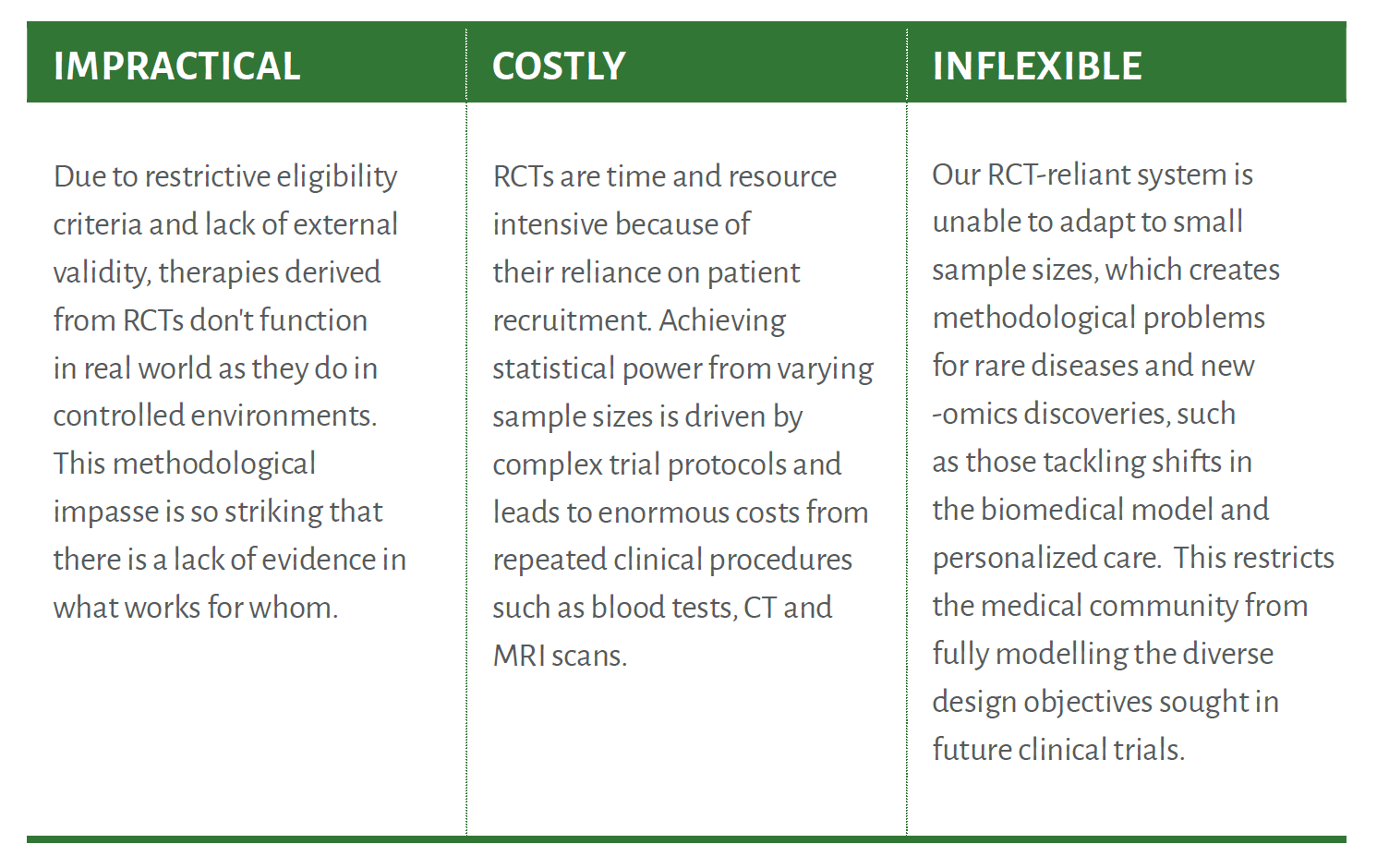
Randomized Controlled Trials (RCTs)—a methodological example of the frequentist approach— dominate the hierarchy of evidence generation due to their stable, systematic approach to clinical experimentation. However, overreliance on one methodology in the treatment development system can result in impractical, costly, and inflexible trials.
There are severe system-wide impacts of generating evidence using predominantly one methodology: today, our RCT-dominated treatment development system is consistent, but inflexible to the evolving needs of human biology. Further, if one methodology dominates evidence generation, other more relevant techniques are less utilized or underdeveloped.
Vision
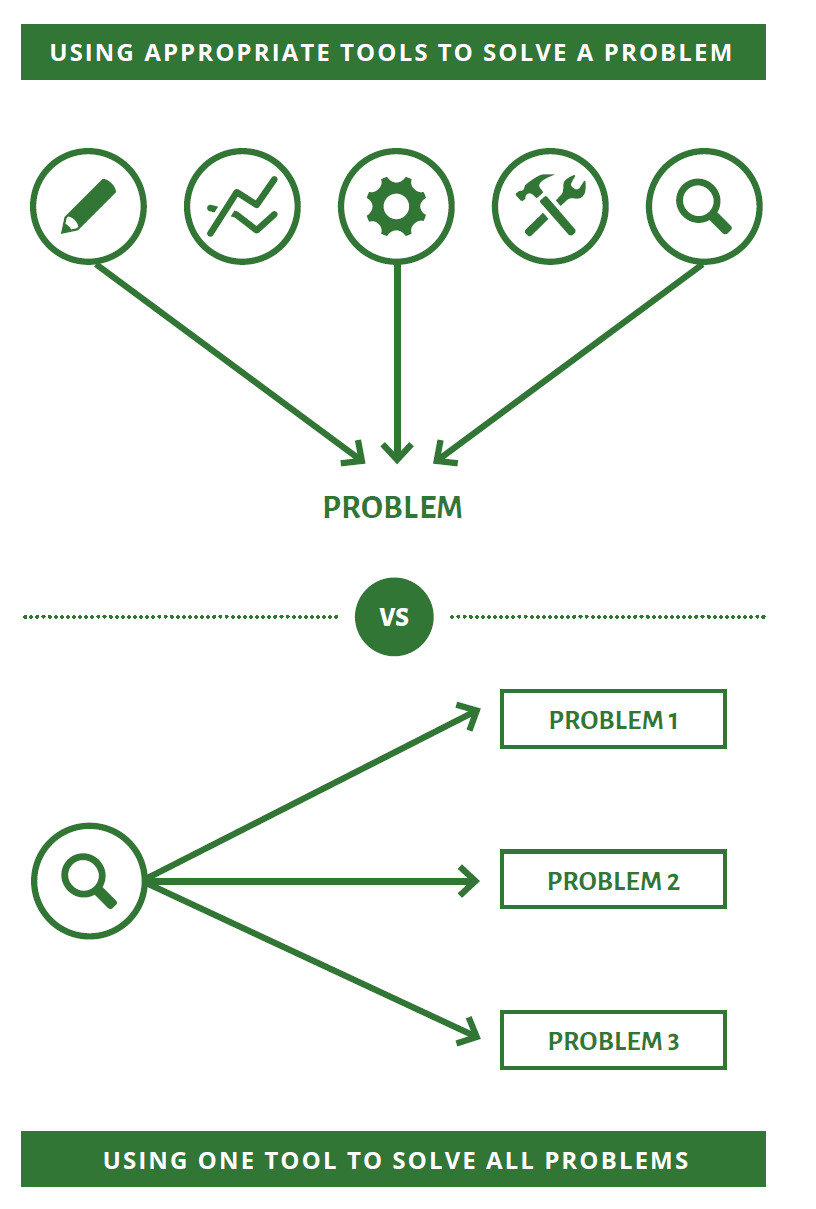
Our vision is that medicine needs more tools in its toolbox. Twinning the medical and mathematical communities— clinical trialists and pure mathematicians — will help practitioners within the treatment development system not only imagine ways of better matching treatments to patients, but also of responding to heavy volumes of clinical decisions seen in the world today.
The flexibility of new techniques will bring their own advantages to the regulatory approval process, by being better suited to regulatory decision-making than RCTs. Having a flexible and robust regulatory approval process built on strong evidence generation methods will lead to better outcomes for the general population.
Next Steps
Building a methodological toolbox for the treatment development system will require two fundamental shifts. In the short-term, the medical community must find and make the most of existing — but less used — evidence generation techniques. These include familiar tools such as centralized registries, case studies, and case series, but also less familiar approaches such as causal inference (an active topic in statistics, but often overlooked in mathematics). By bringing together mathematicians, statisticians, and medical researchers we can determine the viability and application of existing methods to spaces where RCTs are impractical, costly, and inflexible. In the long-term, disrupting the current way of doing things will necessitate generation and regeneration of new and different evidence generation methodologies, complete with new depths and breadths of data, specifically necessary for clinical research. We must not only search for new technologies, but embolden medicine to continuously develop its own new methods for evidence generation.